What is a headache: The four most common types of headache. And, can you hurt your brain by thinking too much?
First off, if you’re experiencing the worst headache of your life, please stop reading and head to an emergency room, especially if it’s onset was sudden.
Alright, moving on:
I’ll start with a personal story and get to the studies, below. Feel free to skip ahead.
I was thirteen, in English class and struggling to read. Don’t get me wrong, I knew how to read, but on this particular day, in this particular class, I couldn’t read at all. The center of my vision looked something like this:
“I’m going blind,” I thought, as I strained to read the blurred letters. I’m going fucking blind. I was too embarrassed to raise my hand and ask to go to the nurse. What exactly would I say, if I did? That I’m going blind? I decided to wait it out. Always a smart to wait things out when you’re convinced you’re becoming permanently disabled, right? So, I sat waiting until the end of the period, hoping I wouldn’t get called on to read something.
When the period ended, I bee-lined it for the nurse’s office. On the way, my head began to throb.
“I’m going blind” I told her, expecting her face to fill with worry.
“What do you mean?” She said calmly.
“The middle of my vision is blurry, I can’t read.”
“Do you feel anything else? Do you have a headache?”
“Yes, my head hurts, because I’ve been straining trying to read.”
“Have you ever had a migraine before?”
“No.”
I hadn’t had a migraine before, and I didn’t know why she was so concerned with a headache, while I was going blind. She called my mom, to take me to the doctor’s. As I sat in the nurse’s office, waiting for my mom, who actually was a teacher in the same middle school, the pulsing pain on the right side of my head became the worst headache I’d ever experienced.
The doctor confirmed the school nurse’s suspicion, a migraine with aura. It turns out the blurring in the center of my vision was an aura, or a weird symptom that precedes the onset of some migraines or seizures. Visual ones can range from the blurred distortions I experienced to more psychedelic distortions, like this artist’s depiction:
From wiki. Sorry about this jarring, headache-inducing image! If it bothers you, scroll down so it’s off the page.
My middle school migraine is so far the only one I’ve experienced. In fact for me, headaches in general pretty much disappeared in high school. Sometimes I wonder if it was just from getting older, from running track and cross country, or a habit that accompanied running–conscientiously drinking water throughout the day.
In college, headaches came back, but this time it was my fault: caffeine withdrawal headaches. I’ve found though, I only get them if I drink coffee immediately after waking up. Since then, I’ve switched my habits so I don’t drink coffee until after my morning commute. Even though I drink just as much caffeine as in college, on days I can’t get my coffee, I may be tired and groggy, but the withdrawal headaches have gone away.
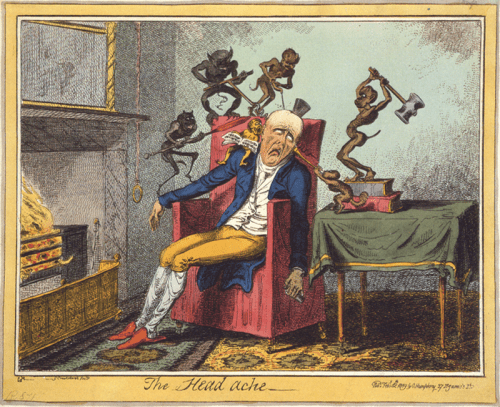
An 1819 caricature by George Cruikshank depicting a headache, via wiki.
The four main types of headaches
Now I want to shift away from anecdotes, and into the evidence. What are headaches?
Headaches may sound like minor inconveniences, but they cause more disability than any other neurologic problem.[1] In fact headaches are the most common health problems in the world, after cavities.[2]
Four main types of headaches are thought to account for up to 90% of all headaches:[3] migraines, tension headaches, cluster headaches, and chronic daily headaches.
1. Migraines – Migraines tend to only affect one side of the head, and cause moderate-to-severe pulsating pain lasting between four hours and three days. They can be preceded by an aura that can be visual, as I described above, or that can affect other senses, movement, or even language. Sometimes migraines can cause just the aura, and not the full headache. Also, migrates may cause nausea and vomiting.
Migraines can be brought on by certain triggers (though nocebo effects may be involved). Based on patient accounts, these are the top 10 most common migraine triggers:[4]
| Trigger | Percent reporting as trigger |
| 1. Stress | 79.7% |
| 2. Hormones (in women) | 65.1% |
| 3. Not eating | 57.3% |
| 4. Weather | 53.2% |
| 5. Sleep Disturbance | 49.8% |
| 6. Perfume or odour | 43.7% |
| 7. Neck Pain | 38.4% |
| 8. Lights | 38.1% |
| 9. Alcohol | 37.8% |
| 10. Smoke | 35.7% |
Chronic migraines can be quite disabling, so sometimes patients take medications to try to prevent them. A class of medications known as Beta-blockers (which often used to treat hypertension) are also strongly recommended, as well as some tricyclic antidepressants, anti-seizure medications, and interestingly, commercially-produced proprietary herbal butterbur extract (though there are serious concerns that butterbur may contain other chemicals that are toxic to the liver). Different sets of drugs are used to abort migraines right as they are beginning and treat their symptoms after they start.
The cause of isolated migraines without auras remains unknown, but we know a lot about migraines with auras.

from Tfelt-Hansen, 2009
Migraines with auras are are associated with a decrease in blood flow in an area of the cortex that spreads outwards from that point, as well as a cortical spreading decrease in brain activity. Some types of migraines with auras run in families, and therefore have genetic components.
In many cases, it is still unknown which genes are involved in these familial migraines, but some migraine-linked genes have been identified. For example mutations to sodium channels, calcium channels, and the Na/K+ATPase cause familial hemiplegic migraine syndromes, which suggests that the level of neural excitability is important for these syndromes.[5]

I haven’t read it yet, but Oliver Sachs devoted an entire book to the migraine. (See which of his books made their way onto the top five books about neuroscience that changed my life.)
2. Tension Headache – Tension headaches are probably what you think of when you think of a run of the mill headache. Every year, up to 65% of people will experience a tension headache,[6] with people in their 30s experiencing the most tension headaches.[7] They are mild or moderate, non-throbbing headaches, that usually respond to anti-inflammatory drugs like ibuprofen. However, be careful, many people who get tension headaches chronically (15 or more days per month) end up overusing these acute medications, which can make the problem worse in the long run.
It’s still unclear to what extent tension headaches are from pain in face and head muscles and to what extent they originate from pain-processing regions of the brain itself. Many neurologists now believe that the occasional isolated tension headache may be muscular in origin, whereas chronic tension headaches may originate from within the brain.[8]
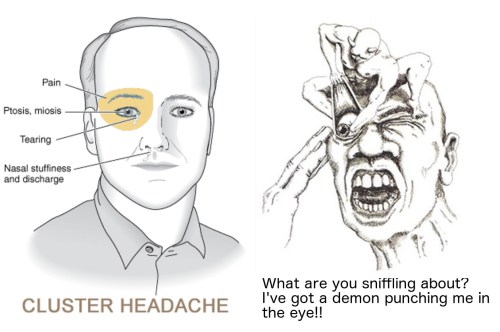
Two very different artist’s depictions of cluster headaches.
3. Cluster Headaches – Only one in a thousand people will get a cluster headache in their life,[9] with the average age for a first cluster headache at 31. Cluster headaches cause severe pain to one side of head for 15 minutes – 3 hours. They’re called cluster headaches because they occur in bursts, where a sufferer may get the headaches frequently for weeks and months, followed by months to a year without any attacks.
The severe headache may be accompanied by tearing, sweating, swelling, nose running, on the same side of the face that the headache is experienced.
Acutely, cluster headaches can respond to breathing 100% oxygen, and certain anti-migraine drugs. To prevent cluster headaches from occuring, verapimil, a calcium channel blocker is recommended.
The exact cause of cluster headaches is unknown, but smoking is a known risk factor, and there is a genetic component as well, with as around 11% of sufferers who have a direct relative (much higher than would be expected because the condition is so rare).
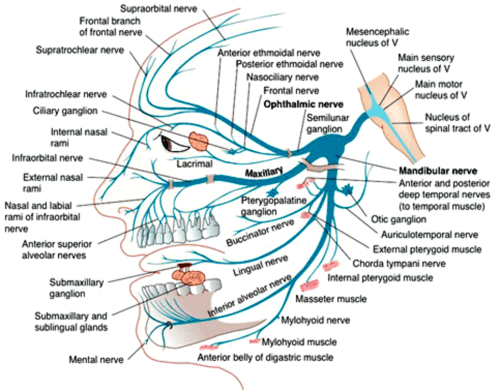
Cluster headaches may involve over-activation of nerves or abberant activity in the brain. Studies have shown increased activity in the opthalmic division of the trigeminal nerve, and altered hypothalamic activity, and some patients can even be treated through hypothalamic deep brain stimulation).[10]
4. Chronic Daily Headache – Despite it’s name, chronic daily headaches aren’t always experienced every day. This diagnosis is given to people who experience 15 or more headaches per month. Chronic daily headache is more of a catch-all category than it’s own specific disease, and in fact, if you experience one of the previously mentioned headaches often enough, e.g. you get tension headaches twenty days each month, these headaches may be reclassified as chronic daily headaches.
Can you hurt your brain by thinking too much?
People often say that the brain is like a muscle, and while it’s true that many skills and memories are similar to muscles in that you need to ‘use them or lose them,’ the metaphor falls apart quickly after that. The brain itself doesn’t contain pain receptors, so a headache is not any indication that your brain is in pain (though the blood vessels and dura coating the brain contain pain detectors that can activate you if you brain is swollen or infected).
As far as we know you can’t damage your brain from thinking too much. Brain cells themselves become over active, that can damage them—a process called excitotoxicity— but this is only thought to occur in situations like epilepsy, drug abuse, or overstimulation by other dying cells. In fact there appears to be no change in the overall level of brain activity between someone concentrating full force and someone sitting idly and letting their mind wander.
But while over-thinking may not hurt your brain, over-thinking may make your head ache. As we saw above with migraines can be triggered by stress, not eating, and sleep disturbances, and tension headaches are also associated with stress, mental tension, or emotional disturbances. And working or studying too hard to an extreme may be counter-productive, as practices like meditation, which I think of as a kind of deliberate rest for many of your over-active brain circuits, has been shown to have lots of long-term benefits.
A final aside
There is one rare situation, where if you’re unlucky overuse of certain brain circuits may cause them to dysfunction: focal dystonia. This is a disease is sometimes called writer’s cramp, but most people don’t actually understand what writer’s cramp means, so that shorthand isn’t very useful. In this disease, ironically, the specific circuits for a motor skill that you spend years and years learning or using, becomes damaged.
From wikipedia: ”Focal dystonia most typically affects those who rely on fine motor skills (musicians, writers, surgeons, etc.). It is thought that the excessive motor training in these individuals may contribute to the development of dystonia as their cortical maps become enlarged and begin to overlap.[8] Focal dystonia is generally “task specific,” meaning that it is only problematic during certain activities.”
However, it is unclear if the overuse is actually causing some sort of real brain damage (such as a loss of neurons), or if rather, it results from a mis-wiring or aberrant activity within the existing circuit, for example that cortical map overlap mentioned in the wikipedia article.
If you liked this blog post and want to read more like it, please share it. If you didn’t like it, leave me some feedback. (Sometimes it feels like I’m just writing into a void.)
References (sorry, for the sloppy citation style, but the citations are legit):
[1] Harrison’s Internal Medicine, 19e, Chapter 21.
[2] The Global Burden of Disease survey 2010, Lifting The Burden and thinking outside-the-box on headache disorders http://www.l-t-b.org/assets/43/4F3BA7B2-DAF8-4C4B-A882874414B2341B_document/Outside_the_box.pdf
[3] http://www.uptodate.com/contents/evaluation-of-headache-in-adults
[4] The triggers or precipitants of the acute migraine attack http://onlinelibrary.wiley.com/doi/10.1111/j.1468-2982.2007.01303.x/full
[5] http://journals.sagepub.com/doi/pdf/10.1177/0333102413485658
[6] http://www.uptodate.com/contents/evaluation-of-headache-in-adults
[7] https://www.ncbi.nlm.nih.gov/pubmed/9459472?dopt=Abstract
[8] Tension-type headache: current research and clinical management – http://www.thelancet.com/journals/laneur/article/PIIS1474-4422(07)70325-3/abstract
[9] http://www.uptodate.com/contents/cluster-headache-epidemiology-clinical-features-and-diagnosis?source=see_link§ionName=EPIDEMIOLOGY&anchor=H3#H3
[10] Cluster headache: pathogenesis, diagnosis, and management. https://www.ncbi.nlm.nih.gov/pubmed/16139660?dopt=Abstract
Filed under: Uncategorized | 2 Comments
-

Subscribe via RSS
Current Neuroscience Book Recommendation:
In Search of Memory -Eric Kandel
Kandel’s book is a nobel prize winner's memoir that spans from his Jewish childhood in Nazi-occupied Vienna to his work on sea slugs that uncovered synaptic plasticity, the molecular foundation of learning and memory. When I graduated college, every neuroscience major was given a copy of this book.


This author says he’s had caffeine withdrawal headaches, yet he doesn’t include caffeine withdrawal headache on his list of four types of headache.
The author also had migraine with aura. My view is that the author’s migraine with aura episodes and caffeine withdrawal headache episodes are manifestations of one highly-variable condition that has been mistaken for multiple, distinct and separate conditions. In my view, he has *primary headache*, which includes migraine with aura, migraine without aura, tension-type headache, cluster headache, and, yes, caffeine withdrawal headache. In my view primary headache and caffeine withdrawal headache are one and the same condition.
Migraine and other types of primary headache have never been demonstrated to occur absent caffeine use; caffeine abstinence has never been verified in a primary headache patient.
My other comments:
Advancement in the scientific understanding of migraine has rendered Sack’s Migraine book obsolete.
The author writes: “Many neurologists now believe that the occasional isolated tension headache may be muscular in origin, whereas chronic tension headaches may originate from within the brain.”
[me] Those neurologists are wrong. Headache researchers years ago demonstrated that muscles are not more tense during tension-type headache episodes than between them. Nor does headache originate within the brain. (To his credit the author acknowledges elsewhere that headache *pain* does not originate within the brain.)
Triggers:
**Stress**
“Stress” associated with headache seems to entirely consist of caffeine-caused anxiety. It’s not
“stress” —> migraine
but rather
anxiety (“stress”) caffeine withdrawal —> severe headache (migraine).
**Hormones**
Estrogen influences caffeine withdrawal headache by inhibiting caffeine metabolism. This mechanism could account for why most migraine patients are women, and account for headache associated with female reproductive events.
**Not eating**
If skipping a meal involves skipping a dose of caffeine, caffeine withdrawal headache may result.
Also: it may be this is mistaking a symptom of migraine — loss of appetite — for a migraine trigger.
**Weather**
Weather influences caffeine intake by encouraging or discouraging the consumption of caffeine-containing beverages.
**Sleep Disturbance**
insomnia caffeine withdrawal —> severe caffeine withdrawal headache (migraine).
**Perfume or odor**
This is another case of effect (symptom) being mistaken for a cause. Migraine can cause olfactory aura: odors are amplified or distorted. Typically in a migraine episode the aura phase precedes the headache phase. Patients can notice and remember a strange or strong odor, and mistakenly conclude the odor caused or triggered the associated headache. (*Post hoc* error.)
**Neck Pain**
Migraine symptom rather than a cause.
**Lights**
Photophobia (excessive sensitivity to light) is a migraine symptom. But light can also aggravate migraine symptoms. So light is both a symptom and an aggravating factor.
**Alcohol**
Aggravating factor. Never been demonstrated to cause a headache in any person absent caffeine use / caffeine withdrawal.
**Smoke**
Cigarette smoking induces caffeine metabolism, so makes caffeine withdrawal headache more likely to occur.
LikeLike
I have heard about the oxygen resolution to cluster headaches for awhile now, but at the time I heard it, it was still in a theoretical stage and hadn’t been proven 100%. I even recommended it to a friend who suffered from cluster headaches to ask her GP about.
LikeLike